Segmentation of lung tumours by deep learning
SummaryPermalink
Lung tumors are a major public health issue. This project is part of a global project on the characterization of lung tumors by machine learning using radiomics techniques. For this, we need to automatically segment these tumors on CT images. To segment these lung tumors, we will use deep learning which currently gives the most accurate results in terms of quality, robustness, and computation time. In particular, we will focus on developing memory-efficient neural networks that can process large 3D images in a single pass through the network, without slicing them into thumbnails.
The dataPermalink
The data we use are public data from The Lung Image Database Consortium image collection (LIDC-IDRI) available on the internet here. These data were collected through a collaboration of seven academic and eight image centers. These data consist of 1018 CT cases and their XML annotations totaling 130 GB.
Methods used for the segmentation of LIDC-IDRI tumours:Permalink
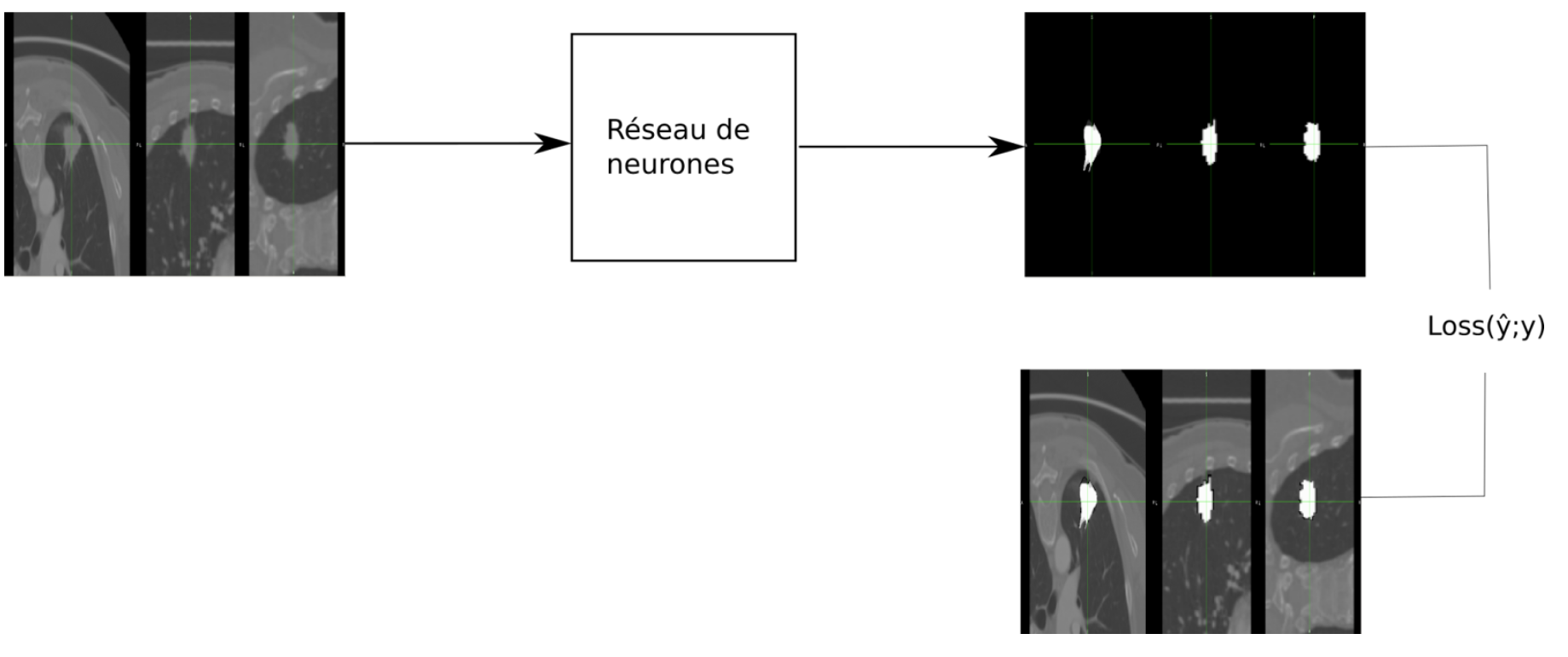
The neural network is used to segment a lung image to segment lung tumors. The goal is to minimize the loss between the annotated segmentation map and the one automatically segmented by the neural network.
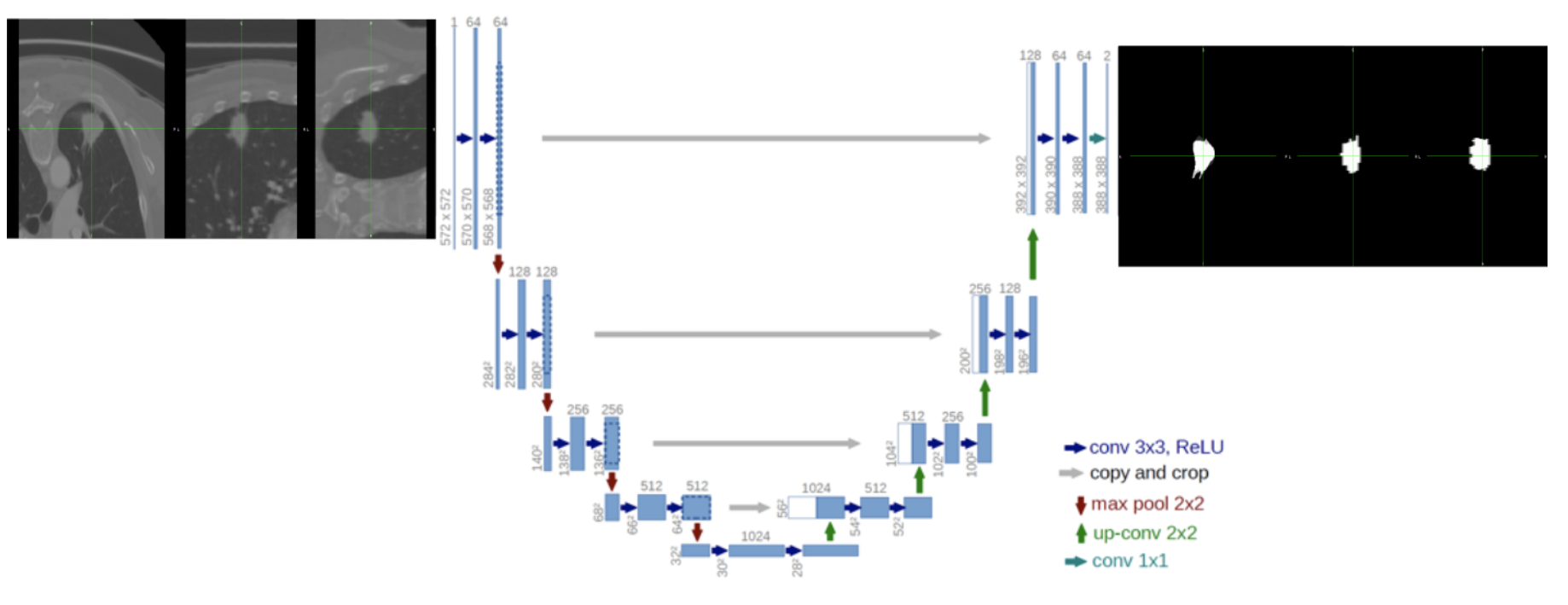
In the state of the art, we find the UNet is a deep learning architecture with high performance for medical image segmentation.
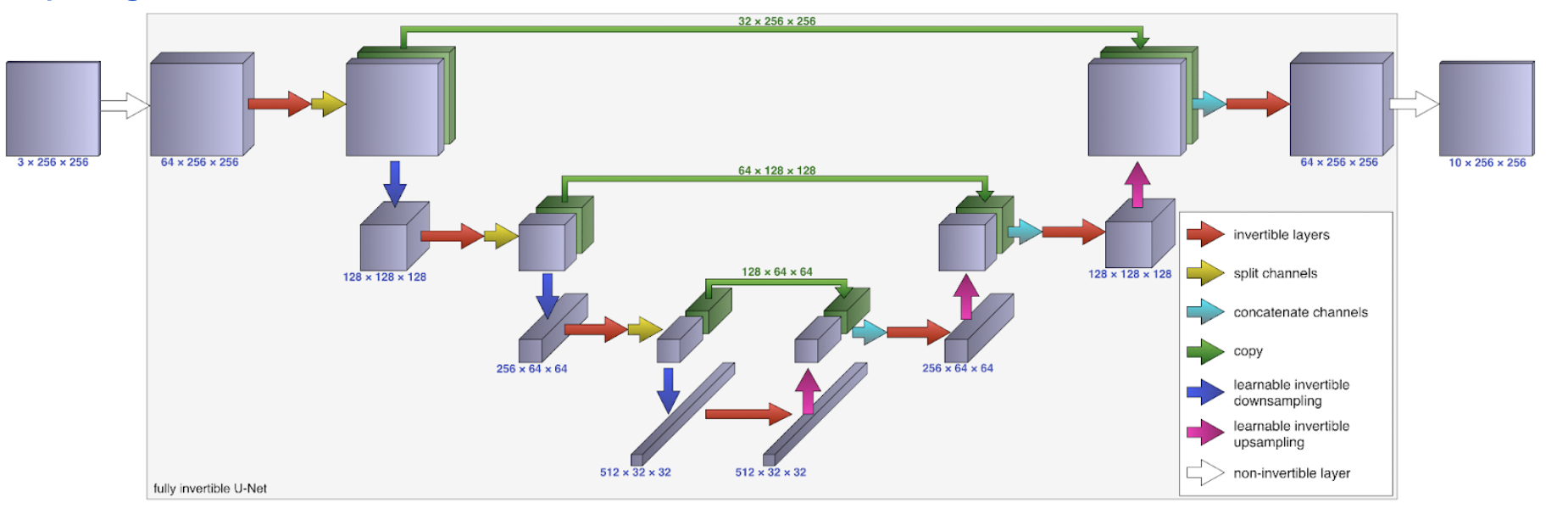
Therefore, this architecture (UNet) requires a lot of memory resources for large data such as 3D medical images. An alternative to solving this problem is to optimize the algorithm by allowing memory-efficient back-propagation. An architecture called iUNets:
- Fully invertible U-Nets with Learnable Up and Downsampling have been proposed by Etmann, C., R. Ke, and C.-B. Schönlieb (2020). Iunets: Fully invertible u-nets with learnable up- and downsampling.
- The source code is also available here.
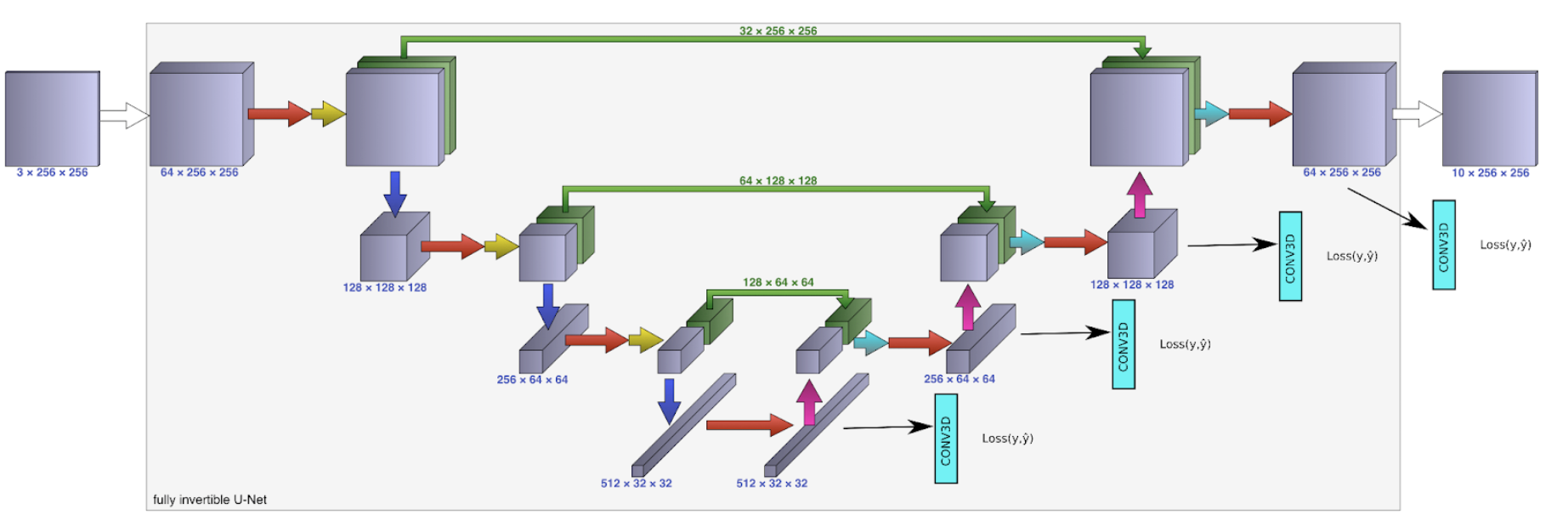
An alternative approach with multi-scale loss calculation and weighting on each scale (given the state of the art
- Krebs, J., H. Delingette, B. Mailhe, N. Ayache, and T. Mansi (2019). Learning a probabilistic model for diffeomorphic registration. IEEE Transactions on Medical Imaging 38 (9), 2165-2176.)
was developed with iUNets and tested with tumor segmentation on 3D images.
Segmentation results of the LIDC-IDRI tumours:Permalink
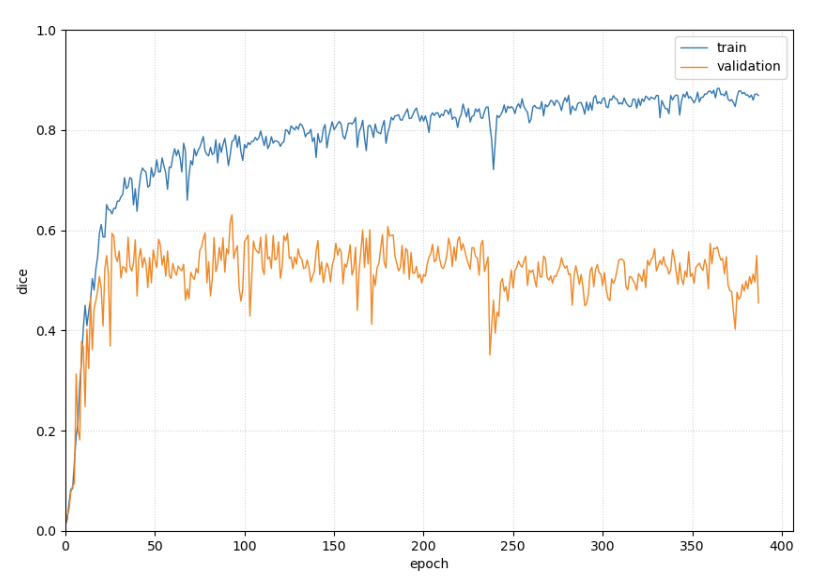
To evaluate our results, we look at the dice curves (a measure of similarity between the true segmentation map and the one found by machine learning) for training (80% of the data) and validation (20% of the data). All three approaches are applied to the cropped images (the tumor is placed in the center of the image) of the LIDC-IDRI.
Figure 4 is an example of these results, obtained by the iUNet. We notice that at 50 epochs we start to overlearn on the training base at the same time as on the test base we are slightly down on the dice curve.
For this purpose, we tried to improve the iUNet architecture with a multi-scale loss calculation and weighting. The results obtained with these two methods by adding a multi-scale loss calculation can be seen in Figure 5. The dice curve for the validation goes down less than in the case of iUNets.
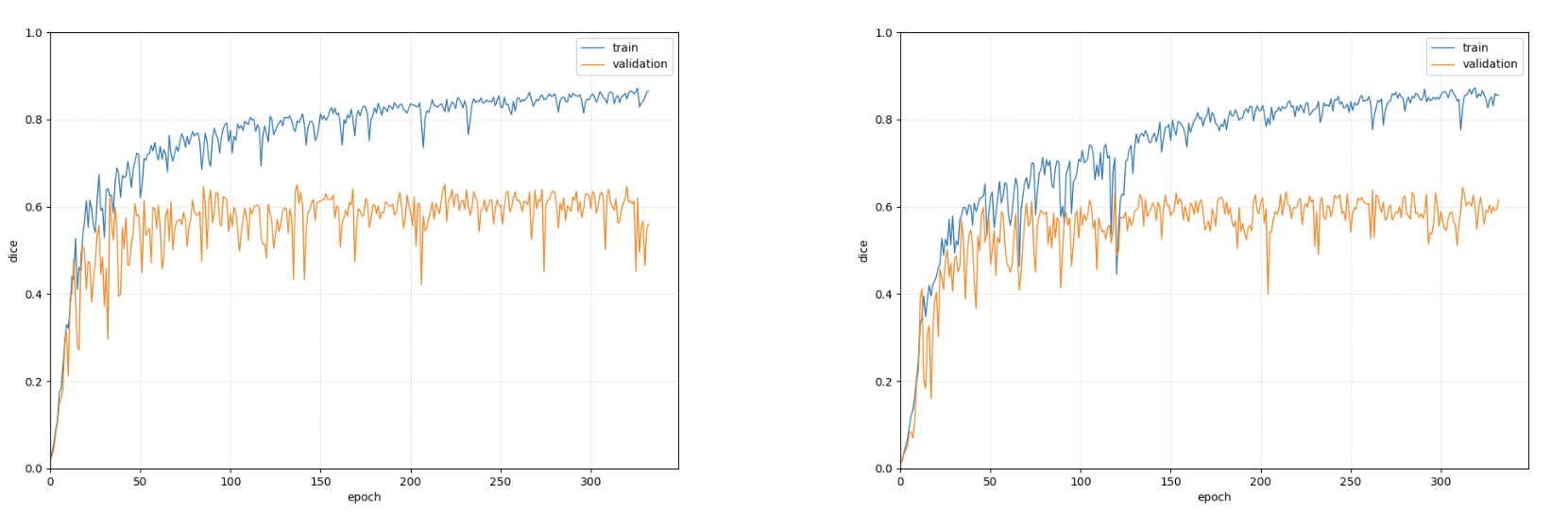
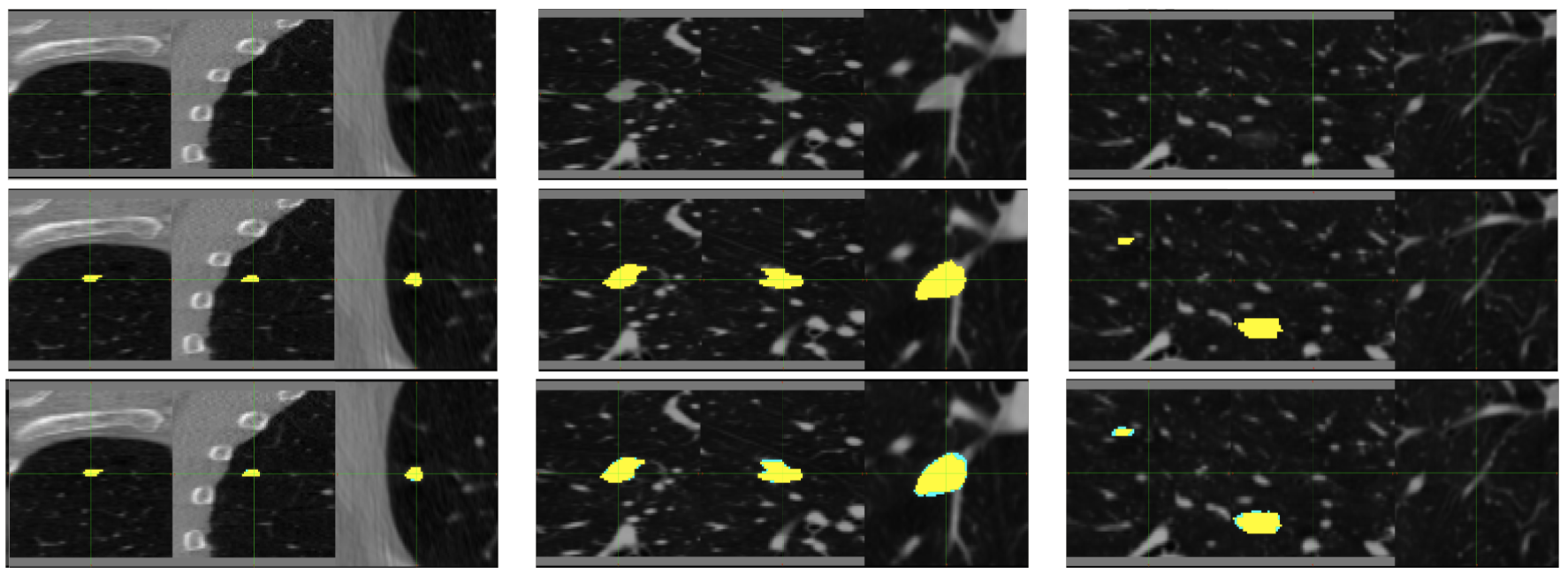
Figure 6 shows the LIDC-IDRI cropped lung images (tumors are placed in the center of the image) (top); the annotated segmentation map (middle); and the tumor segmentation with iUNet and multi-scale loss calculation (bottom).
Objectives and perspectives:Permalink
The results shown in figure 6 are quite accurate in terms of automatic segmentation. We observe that the annotated segmentation map and the one found by the neural network are different on the border. However, its images are cropped with the tumor in the center of the image and the model does not fit the whole image. The results are not good enough when learning this neural network on whole images. The next step in this work will be to perform tumor detection using a neural network and to use the results for segmentation.